

Mito Essential Panel
A simple yearly baseline to confirm the essentials are on track and catch anything drifting early.
Consider this test if:
- You want an affordable yearly baseline you can track year over year
- It has been more than a year since your last full blood work
- You feel well and want a broad, low-cost check that nothing is drifting
- Investigating fatigue, weight change, or low energy and you want a wide first look
- Family history of heart disease, diabetes, or thyroid problems
- HSA/FSA eligible
- Most results within 3 days · Reviewed by a real clinician
- Drawn at a CLIA/CAP-accredited lab near you ·
Pre-test considerations
Fasting 9 to 12 hours is recommended for accurate glucose and lipid results; water is fine. Morning draws are standard. Note any supplements or medications you take, since some can shift individual markers.

Video consult with your Care Team
A 1:1 call to discuss your health.
What members say on Trustpilot
What this test is for
The Mito Essential Panel is the simplest way to set a yearly health baseline and start paying attention before you have to. A single blood draw covers cardiovascular risk with Apo B, a thyroid check, the main sex hormones, vitamin D, and inflammation with hs-CRP, alongside the fundamentals of blood sugar and metabolism, a complete blood count, liver and kidney function, and a urinalysis. It answers two questions at once, where your numbers sit today and whether anything is drifting in a direction worth a closer look. Because it spans several systems rather than one, it works best as an annual checkpoint you can compare year over year. When a marker comes back off, it points you toward the specific follow-up worth doing next, whether that is a fuller thyroid workup, iron studies, or a deeper hormone panel.
Biomarkers tested
Heart Health
ApoB counts the actual number of atherogenic particles (LDL, VLDL, and their remnants) circulating in your blood, since each one carries exactly one ApoB molecule on its surface. It's a more accurate readout of cardiovascular risk than LDL cholesterol, because LDL-C measures the cholesterol cargo inside those particles but misses how many particles are actually out there depositing it into artery walls. Testing it matters for anyone building a baseline on heart disease risk, tracking response to diet or statin therapy, or with a family history of early cardiovascular events despite a normal-looking LDL.
- Specimen
- Serum or plasma
- Measures
- Mass concentration
HDL cholesterol measures the fraction of cholesterol carried by particles that pull excess cholesterol out of artery walls and ferry it back to the liver for disposal, a process called reverse cholesterol transport. Low HDL removes less cholesterol from circulation and tracks with higher cardiovascular risk, often alongside high triglycerides, excess visceral fat, insulin resistance, or a sedentary lifestyle. Checking it alongside ApoB and triglycerides gives a fuller risk picture than total cholesterol alone, and it's a useful marker for tracking how exercise, weight loss, or alcohol reduction shift your lipid profile over time.
- Specimen
- Serum or plasma
- Measures
- Mass concentration
LDL cholesterol refers to the cholesterol carried by LDL particles, the ones that lodge in artery walls and seed plaque. High LDL is the classic driver of atherosclerosis and a core input for cardiovascular risk, useful as a baseline and for tracking response to diet, exercise, or statin therapy. Because it's calculated rather than directly measured, it loses accuracy when triglycerides run high, which is when a direct LDL or ApoB test tells you more.
- Specimen
- Serum or plasma
- Method
- Calculated
- Measures
- Mass concentration
Total cholesterol adds up everything your blood carries: LDL, HDL, and a fraction of your triglycerides. It's a decent starting snapshot but a blunt one, since it can't tell you whether the load is mostly protective HDL or the LDL particles that drive plaque, which is why it's best read alongside ApoB or an LDL/HDL breakdown rather than on its own. Useful as a baseline cardiovascular check or to track how diet, weight change, or medication are shifting your lipid picture over time.
- Specimen
- Serum or plasma
- Measures
- Mass concentration
Triglycerides measure the fat circulating in your blood after your body packages up unused calories, mostly from carbs and alcohol, for storage. High levels signal that your liver is overwhelmed with fuel it can't burn, a pattern common with excess sugar, alcohol, weight gain, or insulin resistance, and one that drives cardiovascular risk independent of LDL. Pair it with fasting insulin and HDL to see the full metabolic picture, and track it when you cut sugar, alcohol, or refined carbs to see if the intervention is actually working.
- Specimen
- Serum or plasma
- Measures
- Mass concentration
VLDL cholesterol tracks the cholesterol packed into VLDL particles, the fat-and-triglyceride carriers your liver ships out to deliver energy to tissues. This value is calculated (typically triglycerides divided by 5), so it rises whenever triglycerides run high, flagging excess liver fat production often tied to insulin resistance, weight gain, alcohol intake, or a high-sugar diet. Elevated VLDL adds to your atherogenic particle burden alongside LDL, making it useful context for cardiovascular risk and for tracking how diet, exercise, or metabolic treatment are moving your triglycerides over time.
- Specimen
- Serum or plasma
- Method
- Calculated
- Measures
- Mass concentration
Hormonal Health
DHEA-S is made almost entirely by the adrenal glands and serves as a stable reservoir your body converts into testosterone and estrogen as needed, making it a reliable read on adrenal androgen output since it doesn't fluctuate hour to hour like cortisol. Low levels can accompany fatigue, low libido, reduced muscle mass, and mood changes, and often show up with adrenal insufficiency or normal age-related decline, while high levels point toward PCOS or an adrenal disorder and often come with acne, excess hair growth, or irregular cycles. It's a useful baseline for tracking adrenal and hormonal aging over time, and a key piece alongside testosterone and cortisol when investigating unexplained fatigue or hormonal symptoms.
- Specimen
- Serum or plasma
- Measures
- Mass concentration
Estradiol is the dominant estrogen, produced mainly by the ovaries, and it governs the menstrual cycle, builds the uterine lining, supports bone density, and helps regulate mood and sleep. In women, this test tracks ovarian reserve and cycle phase, monitors fertility treatment, or investigates irregular periods, hot flashes, night sweats, low libido, or mood shifts around perimenopause and menopause. In men, estradiol is made from testosterone and, when elevated, can drive gynecomastia, low libido, or mood changes, so it's often checked alongside testosterone when those symptoms show up or when starting hormone therapy.
- Specimen
- Serum or plasma
- Measures
- Mass concentration
Free testosterone is the small unbound fraction, roughly 1-2% of total testosterone, that's actually available to enter cells and act on muscle, brain, bone, and libido. Total testosterone can look normal while free testosterone runs low if sex hormone binding globulin is high, so this is the number that best explains low libido, fatigue, poor recovery, mood flatness, or difficulty building muscle despite training hard. It's also the marker to track if you're on testosterone therapy or optimizing training and body composition, since it reflects the hormone your tissues actually see, not just what's circulating in reserve.
- Specimen
- Serum or plasma
- Measures
- Mass concentration
The free T4 index is a calculated estimate of active, unbound thyroxine, correcting for the binding proteins that can distort total T4 readings and give a cleaner read on how much thyroid hormone is actually available to your tissues. Doctors use it as a backup or alternative to direct free T4 when protein levels are shifting, from pregnancy, oral estrogen, liver disease, or acute illness. Low values point toward hypothyroidism, with fatigue, weight gain, cold intolerance, hair thinning, and constipation, while high values point toward hyperthyroidism, with anxiety, palpitations, heat intolerance, and unintended weight loss, and either result is best interpreted alongside TSH.
- Specimen
- Serum or plasma
- Method
- Calculated
- Measures
- Mass concentration
SHBG is a liver-made protein that binds testosterone and estradiol, controlling how much hormone is free to act on tissue rather than locked up in transit. High SHBG (common with high estrogen, hyperthyroidism, or liver disease) can leave you hormonally starved even when total testosterone looks normal, while low SHBG (seen with insulin resistance, obesity, or hypothyroidism) inflates free hormone activity. Pairing SHBG with total testosterone gives you an actual free testosterone picture, useful for investigating low libido, fatigue, mood changes, or irregular cycles, and for tracking how weight loss or metabolic changes are shifting your hormone availability over time.
- Specimen
- Serum or plasma
- Measures
- Substance concentration
T3 resin uptake doesn't measure thyroid hormone directly. It measures how much binding capacity is left on thyroxine-binding globulin (TBG), the protein that carries thyroid hormone through your blood, by seeing how much added radiolabeled T3 gets picked up by a resin instead of binding to TBG. Doctors pair it with total T4 or T3 to calculate a free thyroxine index, which corrects for conditions like pregnancy, estrogen use, or liver disease that raise or lower TBG and can otherwise make thyroid results look abnormal when actual hormone activity is normal, useful when thyroid symptoms like fatigue, weight change, or temperature sensitivity don't match your TSH.
- Specimen
- Serum or plasma
- Measures
- Number fraction (%)
Total T4 measures all the thyroxine circulating in your blood, both the small free fraction that acts on cells and the larger portion bound to carrier proteins. Because binding proteins shift with pregnancy, estrogen, and liver or kidney conditions, total T4 can rise or fall without your actual thyroid function changing, which is why it's usually read alongside TSH and free T4 rather than alone. It's most useful for catching those binding-protein effects and rounding out the picture when TSH looks off but the cause isn't yet clear.
- Specimen
- Serum or plasma
- Measures
- Mass concentration
Total testosterone measures the hormone your testes (or ovaries and adrenal glands in women) produce to drive libido, muscle mass, bone density, energy, and mood. Low levels show up as fatigue, low sex drive, harder recovery from training, mood changes, and difficulty building or keeping muscle, while high levels in women can signal PCOS or point to an androgen-secreting source. It is the standard baseline for anyone tracking hormonal health with age, evaluating symptoms, or checking response to training, weight loss, or testosterone therapy.
- Specimen
- Serum or plasma
- Measures
- Mass concentration
TSH is the pituitary's signal to the thyroid, rising when it senses too little thyroid hormone in circulation and falling when there's too much. High TSH points to an underactive thyroid, often behind fatigue, weight gain, cold intolerance, constipation, dry skin, and low mood. Low TSH points to an overactive thyroid, showing up as anxiety, racing heart, weight loss, heat intolerance, or sleep trouble, and it's the single most sensitive marker for catching thyroid dysfunction before it fully unravels your energy, weight, and cycle.
- Specimen
- Serum or plasma
- Measures
- Concentration
Blood Health
- Specimen
- Whole blood
- Method
- Light microscopy
- Measures
- Presence / threshold
- Specimen
- Whole blood
- Method
- Light microscopy
- Measures
- Presence / threshold
Band neutrophils are immature neutrophils released early from the bone marrow when the body needs backup fast, still finishing their development while already heading out to fight infection. A normal count means the marrow isn't under pressure. An elevated count, often called a left shift, signals an active bacterial infection, inflammation, or significant physical stress and often shows up alongside fever, fatigue, or a suspected infection that needs to be tracked down.
- Specimen
- Whole blood
- Method
- Automated cell count
- Measures
- Number concentration
- Specimen
- Whole blood
- Method
- Automated cell count
- Measures
- Number concentration
- Specimen
- Whole blood
- Method
- Automated cell count
- Measures
- Number fraction (%)
Blasts are immature precursor cells that normally stay in the bone marrow, maturing before they enter circulation. Finding them in blood is abnormal at any meaningful number and points toward a bone marrow disorder, most seriously leukemia, where the marrow releases these unfinished cells before they are ready to defend, clear, or carry anything properly. This test is used diagnostically, alongside a full blood count and clinical picture, when something else (unexplained fatigue, bruising, infections, abnormal counts) has already raised concern.
- Specimen
- Whole blood
- Measures
- Number concentration
- Specimen
- Whole blood
- Method
- Manual cell count
- Measures
- Number fraction (%)
Elliptocytes are red blood cells shaped like ellipses instead of the usual disc, spotted when a lab technician examines your blood smear under a light microscope. A few can appear normally, but a significant number points to a membrane defect, most often hereditary elliptocytosis, or to iron deficiency, thalassemia, or other bone marrow disorders that disrupt how red cells are built. This test is typically ordered to investigate unexplained anemia, fatigue, or abnormal red cell counts, helping pin down why your red blood cells aren't holding their normal shape.
- Specimen
- Whole blood
- Method
- Light microscopy
- Measures
- Presence / threshold
- Specimen
- Whole blood
- Method
- Automated cell count
- Measures
- Number concentration
- Specimen
- Whole blood
- Method
- Automated cell count
- Measures
- Number fraction (%)
- Specimen
- Whole blood
- Method
- Automated cell count
- Measures
- Distribution width
- Specimen
- Whole blood
- Method
- Automated cell count
- Measures
- Number concentration
Granulocytes, mostly neutrophils with smaller numbers of eosinophils and basophils, are the white cells that rush to sites of infection or injury and attack bacteria and other invaders. This manual count reports what fraction of your white cells are granulocytes, useful for confirming automated counts and getting an accurate read when cell populations look unusual under the microscope. A result outside the expected range points toward active infection, inflammation, or a bone marrow issue and is typically read alongside your full white cell differential rather than on its own.
- Specimen
- Whole blood
- Method
- Manual cell count
- Measures
- Number fraction (%)
Hematocrit measures the percentage of your blood volume made up of red blood cells, the cells that carry oxygen from your lungs to every tissue. Low hematocrit points to anemia and pairs with fatigue, breathlessness, dizziness, or poor exercise tolerance, while high hematocrit can reflect dehydration, high altitude, smoking, or overactive red cell production, and thickens blood in ways that matter for cardiovascular risk. It's a core piece of the complete blood count, useful as a baseline read on oxygen-carrying capacity and for tracking how iron status, training, or altitude exposure are shifting your blood over time.
- Specimen
- Whole blood
- Method
- Automated cell count
- Measures
- Volume fraction (%)
- Specimen
- Whole blood
- Method
- Light microscopy
- Measures
- Presence / threshold
Immature granulocytes are young neutrophils, eosinophils, and basophils that bone marrow releases early when it's ramping up production, cells that haven't fully matured before entering circulation. A raised percentage signals the marrow is working overtime, most often because of an active bacterial infection, inflammation, or physiological stress, and it tends to rise before other markers catch up, making it a fast early flag when you're feeling unwell with fever, fatigue, or signs of infection. For proactive tracking, a normal result alongside a routine CBC confirms your marrow isn't under acute strain.
- Specimen
- Whole blood
- Measures
- Number fraction (%)
Large granular lymphocytes are the natural killer cells and cytotoxic T cells that patrol the blood, hunting down virus-infected cells and abnormal cells before they become a problem. This count is rarely ordered as routine screening, it's typically pulled when a full blood count or clinical picture suggests LGL leukemia or a related chronic lymphoproliferative disorder, especially alongside unexplained neutropenia, anemia, or recurrent infections. An elevated count warrants follow-up with flow cytometry to characterize the cell population and confirm what's driving the expansion.
- Specimen
- Whole blood
- Measures
- Number concentration
- Specimen
- Whole blood
- Method
- Automated cell count
- Measures
- Number concentration
- Specimen
- Whole blood
- Method
- Automated cell count
- Measures
- Number concentration
- Specimen
- Whole blood
- Method
- Automated cell count
- Measures
- Number fraction (%)
- Specimen
- Whole blood
- Method
- Light microscopy
- Measures
- Presence / threshold
Mean platelet volume measures the average size of your platelets, the cell fragments that plug injured vessels and stop bleeding. Larger platelets are younger, freshly released from bone marrow, and more reactive, so a high MPV often signals increased platelet turnover from inflammation, iron deficiency, or clotting risk, while a low MPV points to reduced marrow production or older, less active platelets. Paired with your platelet count, MPV helps distinguish why a platelet number is off and adds useful context if you're investigating easy bruising, unexplained clotting, or inflammatory conditions.
- Specimen
- Whole blood
- Method
- Automated cell count
- Measures
- Mean cell volume
Megakaryocytic nuclei are a manual smear finding that flags when the bone marrow cells responsible for producing platelets show up in circulating blood, where they don't belong. Their presence signals marrow stress or a disorder pushing immature cells out early, and it's typically picked up when a blood smear is reviewed to investigate abnormal platelet counts, unexplained bleeding or clotting, or other irregularities on a CBC. This isn't a routine wellness check, it's a targeted microscopy finding your doctor orders to chase down what a standard blood count can't explain.
- Specimen
- Whole blood
- Method
- Light microscopy
- Measures
- Presence / threshold
- Specimen
- Whole blood
- Method
- Manual cell count
- Measures
- Number fraction (%)
- Specimen
- Whole blood
- Method
- Light microscopy
- Measures
- Presence / threshold
- Specimen
- Whole blood
- Method
- Automated cell count
- Measures
- Number concentration
Mononuclear cells are the lymphocytes and monocytes in your differential, the cells that recognize threats, produce antibodies, and clean up debris and dying tissue. This manual count expresses them as a fraction of total white cells, useful for confirming automated differential results or getting an accurate read when abnormal or immature cells make automated counting unreliable. A shifted mononuclear fraction shows up in viral infections, chronic inflammation, and certain blood disorders, and helps explain fatigue, swollen lymph nodes, or a white count that doesn't add up.
- Specimen
- Whole blood
- Method
- Manual cell count
- Measures
- Number fraction (%)
- Specimen
- Whole blood
- Method
- Manual cell count
- Measures
- Number fraction (%)
- Specimen
- Whole blood
- Method
- Manual cell count
- Measures
- Number fraction (%)
- Specimen
- Whole blood
- Method
- Light microscopy
- Measures
- Presence / threshold
- Specimen
- Whole blood
- Method
- Manual cell count
- Measures
- Number concentration
This manual count compares nucleated red blood cells to white blood cells, giving the lab a precise ratio used to correct your white blood cell count when immature red cells are present in circulation. Nucleated RBCs normally stay locked in the bone marrow until they mature and shed their nucleus, so finding them in blood signals the marrow is under stress, pushed out early by severe anemia, hemolysis, bone marrow disorders, or low oxygen states. This isn't a standalone wellness check, it's a technical follow-up your lab runs to keep your white cell count accurate whenever nucleated RBCs turn up on a differential.
- Specimen
- Whole blood
- Method
- Manual cell count
- Measures
- Ratio
- Specimen
- Red blood cells
- Method
- Automated cell count
- Measures
- Mean cell volume
This is a catch-all flag from your automated blood count, capturing unusual cells that don't sort cleanly into the standard white cell categories (neutrophils, lymphocytes, monocytes, eosinophils, basophils). A nonzero result doesn't diagnose anything on its own, it tells the lab's analyzer that something atypical, like blasts, abnormal lymphocytes, or other irregular cells, showed up and usually triggers a manual review under the microscope. If you're already investigating unexplained fatigue, bruising, infections, or a suspicious complete blood count, this value tells you whether a closer look is warranted.
- Specimen
- Whole blood
- Method
- Automated cell count
- Measures
- Number concentration
This captures white blood cells that fall outside the standard five-type differential (neutrophils, lymphocytes, monocytes, eosinophils, basophils), typically immature or atypical cells that an automated analyzer flags but can't cleanly classify. A nonzero count usually prompts a manual smear review to identify what's actually circulating, since it can reflect anything from a reactive response to infection to something that warrants closer hematology follow-up. This isn't a marker people track for wellness purposes, it's a quality flag your lab uses to decide whether your blood needs a closer look.
- Specimen
- Whole blood
- Method
- Automated cell count
- Measures
- Number concentration
- Specimen
- Whole blood
- Method
- Light microscopy
- Measures
- Presence / threshold
This test examines a blood smear under the microscope for parasites that invade red blood cells, most notably the organisms that cause malaria, babesiosis, and related infections. It's the standard workup when someone develops fevers, chills, sweats, fatigue, or a recent travel history to a malaria-endemic region raises suspicion of a blood-borne parasite. A positive result identifies the organism directly, which guides urgent treatment, while a negative result helps rule out parasitic infection as the cause of unexplained fever.
- Specimen
- Whole blood
- Method
- Light microscopy
- Measures
- Identity
Platelet count estimates how many clotting cells circulate in your blood, the fragments that rush to a cut or vessel injury and clump together to form a plug. Low counts (thrombocytopenia) show up as easy bruising, frequent nosebleeds, gum bleeding, or heavy periods, and can stem from bone marrow issues, autoimmune destruction, viral infection, or spleen problems. High counts can signal inflammation, iron deficiency, or a bone marrow disorder pushing out too many, so this is a useful baseline check as well as a first step in explaining unusual bleeding or bruising.
- Specimen
- Whole blood
- Method
- Estimated
- Measures
- Number concentration
- Specimen
- Whole blood
- Method
- Automated cell count
- Measures
- Number concentration
- Specimen
- Whole blood
- Method
- Light microscopy
- Measures
- Presence / threshold
Polychromasia is what a technologist sees under the microscope when young red blood cells, still tinted blue-grey from residual RNA, show up in your blood smear. Their presence tells you the bone marrow is releasing cells faster than usual, typically because it's compensating for blood loss or hemolysis (red cells being destroyed early), or responding to iron, B12, or folate treatment. It's a useful confirmation alongside reticulocyte count when investigating unexplained anemia, fatigue, or pallor, and it helps distinguish a marrow actively regenerating from one that's underproducing.
- Specimen
- Whole blood
- Method
- Light microscopy
- Measures
- Presence / threshold
- Specimen
- Whole blood
- Method
- Manual cell count
- Measures
- Number fraction (%)
- Specimen
- Whole blood
- Method
- Manual cell count
- Measures
- Number fraction (%)
- Specimen
- Whole blood
- Method
- Light microscopy
- Measures
- Presence / threshold
- Specimen
- Whole blood
- Method
- Light microscopy
- Measures
- Presence / threshold
Siderocytes are red blood cells caught holding onto free iron granules instead of packaging that iron properly into hemoglobin, and this count reflects how well your bone marrow handles iron during red cell production. Elevated siderocytes point to impaired iron utilization, seen in sideroblastic anemias, lead exposure, certain myelodysplastic conditions, or after splenectomy (since the spleen normally clears these iron remnants from circulation). This is a specialized follow-up test, not a routine screen: it's ordered when a CBC or iron panel shows an unexplained anemia pattern that needs a closer look at how iron is actually being handled inside developing red cells.
- Specimen
- Whole blood
- Measures
- Number concentration
- Specimen
- Whole blood
- Method
- Light microscopy
- Measures
- Presence / threshold
Stomatocytes are red blood cells that carry a mouth-shaped slit across their surface instead of the usual central dot, a shape change that shows up when a technologist examines your blood smear under the microscope. Their presence points to conditions that disrupt the cell membrane's balance of sodium and potassium, including hereditary stomatocytosis, liver disease, and heavy alcohol use, and can also appear as an artifact of sample handling. This test is typically ordered to help explain unexplained anemia or hemolysis rather than for routine baseline screening, and it works alongside a CBC and reticulocyte count to pin down the cause.
- Specimen
- Whole blood
- Method
- Light microscopy
- Measures
- Presence / threshold
This tells your lab technician whether neutrophils, the white blood cells that engulf and destroy bacteria, show vacuoles (small internal bubbles) when examined under the microscope. Vacuolization signals that neutrophils are under stress, most often from active bacterial infection or sepsis, though toxic exposures and certain bone marrow disorders can produce the same pattern. This isn't a marker you order on its own, it surfaces as a called-out finding on a blood smear when something in your CBC warrants a closer look, and it helps confirm or rule out a significant infectious process.
- Specimen
- Whole blood
- Method
- Light microscopy
- Measures
- Presence / threshold
Variant lymphocytes (also called reactive or atypical lymphocytes) are lymphocytes that have changed shape and activity in response to a viral fight, most often Epstein-Barr virus (mono) but also CMV, hepatitis, or other infections. This percentage flags an active or recent viral immune response and helps explain fatigue, sore throat, swollen glands, or prolonged low energy that a standard white cell count leaves unexplained. A rise here alongside symptoms typically prompts follow-up testing for mono or other viral causes rather than assuming the fatigue is lifestyle-driven.
- Specimen
- Whole blood
- Method
- Automated cell count
- Measures
- Number fraction (%)
Liver Health
GGT is an enzyme concentrated in liver cells and bile duct linings, and it leaks into blood when liver cells are stressed or bile flow is obstructed. It's the most sensitive marker for alcohol-related liver stress and for checking whether an alkaline phosphatase elevation is coming from the liver or from bone. Rising GGT also shows up alongside fatigue, right-upper-abdominal discomfort, or unexplained changes in other liver enzymes, and it's a useful baseline for tracking how alcohol intake, medications, or fatty liver risk are affecting liver health over time.
- Specimen
- Serum or plasma
- Measures
- Enzyme activity
Energy & Metabolism
Albumin is the protein your liver churns out in the largest quantity, and it does double duty: it holds water inside your blood vessels (so fluid doesn't leak into tissue) and ferries hormones, fatty acids, and medications through your bloodstream. Low albumin points to liver disease, kidney protein loss, chronic inflammation, or poor nutrition, and often shows up alongside swelling, fatigue, or unexplained weight loss. Because it reflects both liver production and overall protein status, it's a useful baseline check and a quick way to see whether inflammation or malnutrition is quietly dragging your protein reserves down.
- Specimen
- Serum or plasma
- Measures
- Mass concentration
The albumin/globulin ratio compares your two main blood protein groups: albumin, made by the liver to hold fluid in vessels and carry hormones and nutrients, and globulins, produced largely by the immune system to fight infection and transport other molecules. A low ratio points to liver disease, kidney protein loss, chronic inflammation, or an overactive immune system driving up globulins, while a high ratio suggests low globulin production or an immune system that is underactive. Pair it with total protein, albumin, and liver enzymes to sort out whether fatigue, swelling, or unexplained weight change traces back to your liver, kidneys, or immune activity.
- Specimen
- Serum or plasma
- Measures
- Ratio
- Specimen
- Serum or plasma
- Measures
- Enzyme activity
ALT is an enzyme that lives mostly inside liver cells, where it helps metabolize amino acids. When liver cells get inflamed or damaged, from alcohol, fatty liver, viral hepatitis, or certain medications and supplements, they leak ALT into the bloodstream, making it the most specific marker of liver cell injury on a standard panel. It's worth tracking as a baseline if you drink regularly, use supplements or medications processed by the liver, or carry extra weight, and worth investigating if you have unexplained fatigue, abdominal discomfort, or nausea, since ALT often rises well before symptoms do.
- Specimen
- Serum or plasma
- Measures
- Enzyme activity
AST is an enzyme that lives inside liver cells (and muscle and heart cells too), and it spills into your blood when those cells get damaged. High AST flags liver strain from alcohol, fatty liver, medications, or infection, though muscle damage from intense training can also push it up, which is why it's usually read alongside ALT to pinpoint the source. It's worth tracking as a baseline for liver health, before starting a new supplement or medication, or when investigating fatigue, abdominal discomfort, or unexplained changes in appetite.
- Specimen
- Serum or plasma
- Measures
- Enzyme activity
Calcium does far more than build bone: nerves fire, muscles contract, blood clots, and hormones release only when calcium levels stay in a tight range. This test measures total calcium in serum, which parathyroid hormone and vitamin D regulate together with your bones acting as the reserve tank. High calcium points to overactive parathyroid glands, excess vitamin D, or certain cancers, while low calcium suggests parathyroid or kidney dysfunction, vitamin D deficiency, or poor absorption, and either extreme can drive fatigue, muscle cramps, tingling, brain fog, or irregular heartbeat worth investigating.
- Specimen
- Serum or plasma
- Measures
- Mass concentration
Total CO2 measures the bicarbonate-based buffer your blood uses to keep pH stable, reflecting how your lungs and kidneys balance acid and base. Low levels point toward metabolic acidosis (from kidney disease, uncontrolled diabetes, or chronic diarrhea) while high levels suggest metabolic alkalosis or a compensated respiratory condition, both worth clarifying if you're dealing with unexplained fatigue, rapid breathing, or confusion. It's part of the standard electrolyte panel, so most people track it as a baseline metabolic marker alongside sodium, potassium, and chloride rather than ordering it alone.
- Specimen
- Serum or plasma
- Measures
- Substance concentration
Chloride is the main negative ion in your blood, working alongside sodium and bicarbonate to hold fluid balance, blood volume, and acid-base status steady. Low levels track with vomiting, dehydration, or metabolic alkalosis, while high levels point toward dehydration or metabolic acidosis, often from kidney or GI losses. Ordered as part of a basic metabolic panel, it mainly serves as a baseline check and a way to make sense of symptoms like dizziness, muscle cramps, or persistent fatigue tied to fluid or electrolyte shifts.
- Specimen
- Serum or plasma
- Measures
- Substance concentration
Creatinine is a waste product released as your muscles break down creatine for energy, and your kidneys filter it out of the blood at a steady rate. When creatinine rises, it usually means the kidneys are filtering less efficiently, making it the core marker for kidney function and the basis for calculating eGFR. Test it as a baseline for kidney health, to monitor the impact of blood pressure, diabetes, high-protein diets, or supplements like creatine, or to investigate unexplained fatigue, swelling, or changes in urination.
- Specimen
- Serum or plasma
- Measures
- Mass concentration
Globulin is calculated by subtracting albumin from total protein, capturing the group of proteins your liver and immune system produce, including antibodies that fight infection and carrier proteins that transport hormones and nutrients. High globulin points to chronic inflammation, infection, or an overactive immune system producing excess antibodies, sometimes seen in autoimmune disease or certain blood cancers, while low globulin suggests impaired liver production or immune suppression. Paired with albumin and total protein, it helps clarify unexplained fatigue, recurrent infections, or abnormal liver panels, and gives proactive testers a baseline read on liver and immune protein production.
- Specimen
- Serum
- Measures
- Mass concentration
Glucose measures the sugar circulating in your blood right now, the fuel your cells burn for energy and the hormone insulin works constantly to keep in range. High readings point toward insulin resistance, prediabetes, or diabetes, while low readings can explain shakiness, lightheadedness, irritability, or brain fog between meals. Pair it with fasting insulin or A1c to see whether your body is managing glucose efficiently or working overtime to do it, and use it to track how diet, training, or sleep changes are actually moving your metabolism.
- Specimen
- Serum or plasma
- Measures
- Mass concentration
HbA1c measures the fraction of hemoglobin that glucose has permanently attached to over the roughly three-month lifespan of a red blood cell, giving you an average blood sugar reading rather than a single-moment snapshot. Elevated levels point to prediabetes or diabetes and reflect cumulative glucose exposure that drives vascular damage, so it's a core piece of cardiovascular and metabolic risk assessment even before symptoms appear. It also pairs well with fasting insulin and glucose to track how diet, training, weight loss, or medication are actually changing your metabolic trajectory over time.
- Specimen
- Whole blood
- Measures
- Mass fraction (%)
Potassium regulates the electrical signaling that fires your heart muscle, contracts your muscles, and controls nerve conduction, with cells and kidneys working together to keep it in a tight range. Levels that drift high or low show up as muscle weakness, cramping, palpitations, or fatigue, and can result from dehydration, kidney function changes, certain blood pressure medications, or heavy sweating from training. It's a core piece of any electrolyte or kidney panel, useful for a baseline check and essential context if you're on diuretics, ACE inhibitors, or pushing hard in endurance training where fluid and mineral losses run high.
- Specimen
- Serum or plasma
- Measures
- Substance concentration
Sodium is the main electrolyte outside your cells and it controls how water distributes across your body, keeping blood volume and blood pressure stable while nerves and muscles fire correctly. Low sodium shows up as fatigue, headache, confusion, nausea, or muscle cramps, and points to excess water retention, heavy sweating, certain medications, or kidney and hormone issues, while high sodium usually signals dehydration. It's a core part of any metabolic panel, useful as a baseline check and essential for investigating unexplained fatigue, dizziness, or muscle cramping, especially in endurance athletes or anyone on diuretics.
- Specimen
- Serum or plasma
- Measures
- Substance concentration
Total bilirubin measures the pigment left over when your body breaks down old red blood cells, a job the liver clears by processing it into bile. High levels point to a liver struggling to keep up (hepatitis, fatty liver, bile duct blockage) or red cells breaking down faster than normal, and often show up as yellowing skin or eyes, dark urine, or fatigue. It pairs with ALT, AST, and ALP to pinpoint whether a problem sits in the liver cells, the bile ducts, or upstream in the blood itself, and mildly elevated results with otherwise normal liver panels usually reflect Gilbert's syndrome, a harmless and common genetic quirk.
- Specimen
- Serum or plasma
- Measures
- Mass concentration
Total protein adds up albumin and globulins, the workhorses that hold fluid in your blood vessels, carry hormones and nutrients, and fuel your immune defenses. Low levels point toward liver disease, kidney loss of protein, malnutrition, or poor absorption, while high levels can flag chronic inflammation or dehydration. It's a quick baseline check within a metabolic panel, and if your levels drift off, it usually leads straight to albumin and globulin breakdowns to pinpoint what's driving it.
- Specimen
- Serum or plasma
- Measures
- Mass concentration
Blood urea nitrogen tracks the waste product your liver makes when it breaks down protein, cleared by kidneys that filter it out of circulation. High BUN points to reduced kidney filtration, dehydration, or a high protein intake, while low levels can reflect liver trouble or very low protein diets. Paired with creatinine, it rounds out a kidney function baseline and helps investigate fatigue, swelling, changes in urination, or unexplained shifts tied to diet, hydration, or medication changes.
- Specimen
- Serum or plasma
- Measures
- Mass concentration
Uric acid is the breakdown product of purines from cell turnover and diet, cleared by the kidneys once it's made. High levels mean your body is producing more than it can clear, which crystallizes in joints and causes gout, and independently tracks with hypertension, kidney stones, fatty liver, and metabolic syndrome. Testing it makes sense as a baseline alongside metabolic panels, to investigate joint pain or swelling, or to monitor levels if you're managing diet, alcohol intake, or medications known to raise it.
- Specimen
- Serum or plasma
- Measures
- Mass concentration
Nutrients & Minerals
- Specimen
- Serum or plasma
- Measures
- Mass concentration
Inflammation & Immunity
High-sensitivity CRP measures low-grade inflammation circulating in your blood, well below the threshold standard CRP tests are built to detect. The liver releases CRP in response to arterial inflammation, and elevated levels predict cardiovascular risk independent of cholesterol, making this a key add-on to ApoB or Lp(a) for anyone building a real risk picture or tracking whether diet and training changes are actually lowering inflammation. It also helps explain persistent fatigue, joint aches, or unresolved symptoms when something inflammatory is suspected but not yet identified.
- Specimen
- Serum or plasma
- Method
- High sensitivity
- Measures
- Mass concentration
Urine
- Specimen
- Urine sediment
- Method
- Light microscopy
- Measures
- Presence / threshold
This test counts bacteria per high power field in urine sediment examined under a microscope, a direct look for organisms that shouldn't be living in your urinary tract. Elevated counts point to a urinary tract infection, especially alongside white blood cells, and often explain burning with urination, urgency, frequency, pelvic pain, or cloudy, foul-smelling urine. It's a quick way to confirm or rule out infection when symptoms flare, or to check that a prior UTI has actually cleared.
- Specimen
- Urine sediment
- Method
- Light microscopy
- Measures
- Count per area
This dipstick check flags whether bilirubin, a breakdown product of old red blood cells that your liver normally processes into bile, is leaking into your urine. Healthy urine carries none of it, so a positive result points to conjugated bilirubin backing up into the bloodstream, a sign of bile duct obstruction, hepatitis, or other liver dysfunction. It's a useful piece of the puzzle when you're investigating dark urine, yellowing skin or eyes, pale stools, itching, or unexplained fatigue, and it often shows up on the same strip as urobilinogen for a fuller read on liver and bile flow.
- Specimen
- Urine
- Method
- Test strip
- Measures
- Presence / threshold
This marker counts calcium oxalate crystals seen directly under the microscope in a spun sample of your urine, the same crystal type that forms most kidney stones. Finding them is common and often harmless, but frequent or heavy amounts point to concentrated urine, low fluid intake, or a diet high in oxalate (spinach, nuts, chocolate, tea), and correlate with stone risk over time. It's a useful check if you've had a kidney stone before, get recurrent flank pain or blood in your urine, or want to confirm that hydration and dietary changes are actually reducing your crystal load.
- Specimen
- Urine sediment
- Method
- Light microscopy
- Measures
- Count per area
- Specimen
- Urine sediment
- Method
- Light microscopy
- Measures
- Count per area
This test looks under the microscope at urine sediment to count crystals per high power field, the mineral and salt deposits that form when urine holds more of a substance than it can keep dissolved. Certain crystal types point to specific problems: calcium oxalate and uric acid crystals often accompany kidney stone formation, while others can flag dehydration, diet extremes, or liver and metabolic conditions. It's a useful add-on if you've had flank pain, blood in your urine, or a history of kidney stones, and useful for tracking whether hydration or dietary changes are actually reducing stone-forming risk.
- Specimen
- Urine sediment
- Method
- Light microscopy
- Measures
- Count per area
Granular casts are cylindrical clumps of degenerated cellular material that form in the kidney's tubules and wash out into urine, visible under the microscope during a urine sediment exam. A few granular casts can turn up after hard exercise or dehydration, but larger numbers point to tubular cell injury and often show up in acute kidney injury, dehydration, or chronic kidney disease. This test is useful for investigating unexplained changes in urine output, swelling, rising creatinine, or fatigue, and for tracking kidney recovery after an insult like illness, medication exposure, or a low-flow event.
- Specimen
- Urine sediment
- Method
- Light microscopy
- Measures
- Count per area
This dipstick screen detects hemoglobin in urine, the protein that carries oxygen in red blood cells and, when present in urine, signals that blood is leaking somewhere along the kidneys or urinary tract. A positive result points to causes ranging from kidney irritation, UTIs, kidney stones, or strenuous exercise, to more serious conditions like kidney disease that warrant follow-up. It is a simple way to catch silent urinary tract or kidney issues before symptoms like pain, changes in urination, or visible blood appear.
- Specimen
- Urine
- Method
- Test strip
- Measures
- Presence / threshold
Hyaline casts are protein molds that form in the kidney's tubules and wash into urine, and technicians count them under the microscope during a urine sediment exam. A few are normal, especially after exercise, dehydration, or a fever, so an isolated finding usually needs no action. A high number, particularly alongside protein in urine, reduced output, or symptoms like swelling and fatigue, points toward more concentrated urine or early kidney stress worth tracking with follow-up testing.
- Specimen
- Urine sediment
- Method
- Light microscopy
- Measures
- Count per area
This dipstick test detects ketones spilling into urine when the body burns fat for fuel instead of glucose. It's useful for tracking a ketogenic or low-carb diet, confirming your body has shifted into fat-burning mode, or checking on a fasting protocol. Unexplained positive results paired with high blood sugar, excessive thirst, or fatigue warrant prompt follow-up, since that combination can signal diabetic ketoacidosis rather than diet-driven ketosis.
- Specimen
- Urine
- Method
- Test strip
- Measures
- Presence / threshold
Leukocyte esterase is an enzyme released by white blood cells, and this dipstick test detects it in urine as a marker of inflammation in the urinary tract. A positive result signals that neutrophils have shown up to fight something, usually a urinary tract infection, and often shows up alongside symptoms like burning with urination, urgency, frequency, or pelvic discomfort. It pairs with urine nitrites and a urinalysis to confirm infection and decide whether further culture or treatment is needed.
- Specimen
- Urine
- Method
- Test strip
- Measures
- Presence / threshold
This dipstick reading detects nitrite in urine, produced when certain bacteria (E. coli and other common culprits) convert dietary nitrate into nitrite as they multiply. A positive result signals a likely urinary tract infection and pairs with leukocyte esterase to confirm it, useful when you're tracking down burning urination, urgency, frequency, or pelvic discomfort. It's also a quick proactive check if you're prone to recurrent UTIs and want to catch one early, before it climbs to the kidneys.
- Specimen
- Urine
- Method
- Test strip
- Measures
- Presence / threshold
This measures how acidic or alkaline your urine is, a quick readout of how your kidneys manage acid-base balance and a marker that shifts with diet, hydration, and metabolic state. Persistently low (acidic) urine is linked to kidney stone formation, particularly uric acid stones, while high (alkaline) urine points to certain infections or renal tubular issues and can favor calcium phosphate stones. If you've had kidney stones before, get recurring UTIs, or are dialing in a diet (high protein, keto, or heavy produce intake) and want to see how it's shifting your body's chemistry, this is a fast way to check.
- Specimen
- Urine
- Method
- Test strip
- Measures
- Concentration
This test counts red blood cells per high-power field in urine sediment examined directly under the microscope, catching hematuria that dipstick testing can miss or falsely flag. Elevated counts point toward kidney or urinary tract sources of bleeding: infection, kidney stones, inflammation in the filtering units of the kidney, or irritation anywhere along the bladder and urinary tract. It's useful both as a routine check on kidney and urinary health and for investigating visible blood in urine, unexplained flank pain, or burning with urination.
- Specimen
- Urine sediment
- Method
- Light microscopy
- Measures
- Count per area
Renal epithelial cells line the kidney's tubules, and finding them shed into urine sediment means those tubules are shedding their lining faster than normal. A microscopist counts them per high power field, and elevated numbers point to acute tubular injury, infection, or toxin exposure (from medications, contrast dye, or heavy metals) rather than a bladder or urethral source of blood or protein. This test is most useful when you already have signs of kidney irritation, such as unexplained protein or blood in urine, and need to pinpoint whether the tubules themselves are under stress.
- Specimen
- Urine sediment
- Method
- Light microscopy
- Measures
- Count per area
Specific gravity measures how concentrated your urine is, comparing it to the density of pure water, and it reflects how well your kidneys balance water and dissolved solutes. High values point to dehydration or concentrated urine, while very low values suggest overhydration or a kidney's reduced ability to concentrate urine at all. It's a quick check for hydration status when you're tracking fluid intake around training, and a useful clue when investigating dark urine, low urine output, or unexplained thirst and fatigue.
- Specimen
- Urine
- Method
- Test strip
- Measures
- Specific gravity
This counts squamous epithelial cells shed into urine sediment and viewed under the microscope, cells that line the urethra, vagina, and outer skin rather than the kidney or bladder itself. A high count usually signals that the sample picked up cells from external contamination during collection rather than pointing to disease, which matters for interpreting everything else in the urinalysis correctly. Labs use this count to judge whether a sample is clean enough to trust, so a raised result on a symptom workup (burning, urgency, cloudy urine) often just means a repeat, better collected sample is needed before drawing conclusions about infection or kidney issues.
- Specimen
- Urine sediment
- Method
- Light microscopy
- Measures
- Count per area
Transitional cells line the bladder, ureters, and upper urethra, forming a flexible barrier that stretches as your bladder fills and shields deeper tissue from urine's caustic contents. Finding more than a few under the microscope points to irritation from a urinary tract infection, catheter use, or kidney stones, and persistently elevated or atypical counts warrant a closer look at the bladder lining. This one usually comes up when someone is investigating urinary symptoms like burning, urgency, or blood in the urine rather than as a routine baseline check.
- Specimen
- Urine sediment
- Method
- Light microscopy
- Measures
- Count per area
This measures triple phosphate (struvite) crystals seen under the microscope when a urine sample is examined for sediment. These crystals form in alkaline urine and often point to a urease-producing bacterial infection (commonly Proteus), so finding them alongside symptoms like cloudy urine, urinary urgency, flank pain, or recurrent UTIs helps confirm infection and flags a risk factor for struvite kidney stones. For most people this is a follow-up test rather than a routine baseline, ordered when a urinalysis raises questions about infection or stone risk.
- Specimen
- Urine sediment
- Method
- Light microscopy
- Measures
- Count per area
This test looks for urate crystals in urine sediment under the microscope, a marker of how concentrated your urine is and how acidic your pH runs. Crystals show up when urine is too acidic or too concentrated for uric acid to stay dissolved, conditions that also favor kidney stone formation. If you've had a uric acid kidney stone, gout flares, or unexplained flank pain, this finding connects the dots and often prompts a look at hydration, diet, and urine pH management.
- Specimen
- Urine sediment
- Method
- Light microscopy
- Measures
- Count per area
This records whether urine looks clear, cloudy, or turbid, one of the basic visual checks in a urinalysis. Cloudy urine points to crystals, mucus, white blood cells, bacteria, or excess protein, and often accompanies urinary tract infections, kidney stones, or dehydration. Pairing it with urine color, specific gravity, and microscopy turns a simple visual cue into a fast first read on hydration and urinary tract health.
- Specimen
- Urine
- Measures
- Appearance
Urine color is a simple visual observation, part of a standard urinalysis, that reflects hydration, diet, medications, and sometimes blood or bile in the urine. Pale yellow signals good hydration, while dark amber urine points to concentrated urine and dehydration, and red, brown, or tea colored urine can flag blood, muscle breakdown, or liver issues that warrant a closer look. It's a quick baseline check alongside other urine markers, or a useful clue when investigating unusual fatigue, dark urine, or changes in urination.
- Specimen
- Urine
- Measures
- Color
This dipstick check flags whether protein is spilling into your urine at all, a quick presence or absence read rather than a precise count. Healthy kidneys keep protein locked in the blood, so a positive result signals that the filtering units are leaking and deserves a closer look with a quantitative test like urine albumin to creatinine ratio. It's a useful baseline for anyone tracking kidney health alongside blood pressure or blood sugar, and a natural next step if you've noticed foamy urine, swelling in the legs or eyes, or unexplained fatigue.
- Specimen
- Urine
- Method
- Test strip
- Measures
- Presence / threshold
This test counts white blood cells sitting in your urine sediment under the microscope, cell by cell, per high power field. Neutrophils flood into urine when they're fighting a bladder or kidney infection, so elevated counts point to a urinary tract infection, and can also flag inflammation from kidney stones, an enlarged prostate, or, less commonly, interstitial cystitis. It's the natural next step if you're dealing with burning, urgency, cloudy urine, pelvic or flank pain, or a positive leukocyte esterase on a dipstick, and it's how you confirm an infection is actually clearing after treatment.
- Specimen
- Urine sediment
- Method
- Light microscopy
- Measures
- Count per area
This test counts yeast cells per high power field in urine sediment examined under the microscope, usually as part of a urinalysis. Yeast in urine most often signals a fungal infection (commonly Candida), and shows up more frequently in people with diabetes, recent antibiotic use, or a weakened immune response. Paired with symptoms like burning with urination, urgency, or vaginal or genital irritation, it helps distinguish a yeast infection from a bacterial UTI so treatment actually matches the cause.
- Specimen
- Urine sediment
- Method
- Light microscopy
- Measures
- Count per area

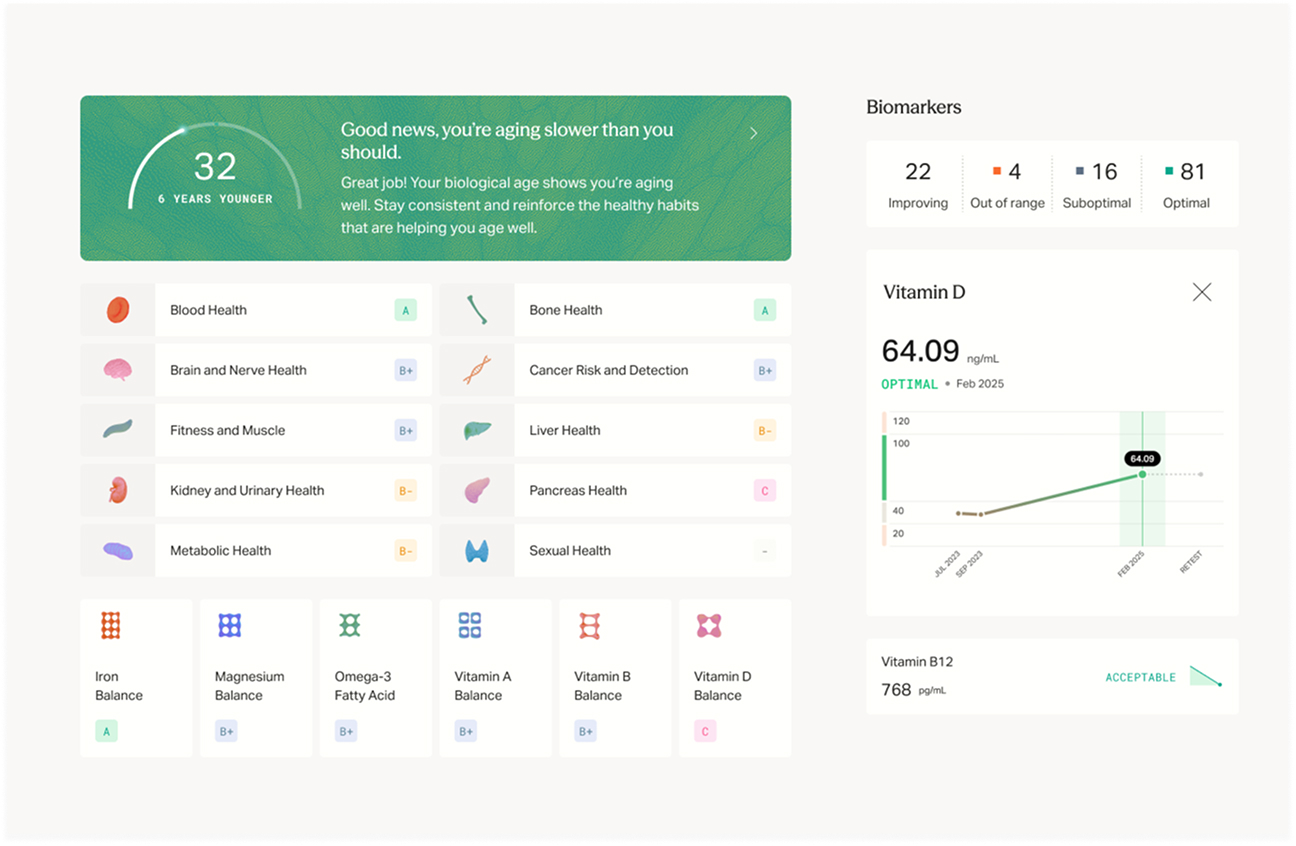
What you'll learn
-
Insights that connect the dots. A clinician reads your whole picture, not one result in isolation, connecting family history, past results, and lifestyle into clear next steps.
-
Your personalized action plan. Nutrition, supplements, and training in one clinician-reviewed protocol, updated as your results change.
-
Track your trends. Upload results from any lab and see each biomarker trend over time, so you know what is working.
-
Never miss a recheck. Mito tells you what is worth retesting and when, then reminds you so nothing slips.
What to expect
- 1 Book instantly
Click, book, done. Choose a convenient lab location near you. Transparent, up-front pricing.
- 2 Quick lab visit
Testing to fit your busy schedule, usually 15 minutes or less. Walk-in and appointments available.
- 3 Most results within 3 days
Your results post straight to your dashboard as soon as the lab completes them.
- 4 Expert guidance
Included with Mito membership. A clinician reviews your results and your personalized action plan follows, with clear next steps.
Everything your health needs,
in one membership
-

Every test at our cost
Members pay our cost on every test, with lab fees passed straight through. The full receipt is itemized, never padded.
-
Continuous tracking, all in one place
Upload past labs and watch your trends over time. Every marker and visit lives in one longitudinal record, so all your care stays together.
-

Year-round clinician support
Text anytime and get clinician-reviewed answers. When you want to go deeper, 1:1 consultations are available at affordable rates.
All for $9/month
Order any test or consult without joining. For $9/month, members unlock member prices, trend tracking, and year-round clinician guidance.
Mito Membership
$9 /mo
cancel anytime
Without membership
$0
pay as you go
At-cost pricing on labs, scans, and more
Supplements at 30% off retail prices Coming soon
On-demand clinician consults when you need guidance
Personalized action plans across supplements, exercise, nutrition, and sleep
AI health coaching to help you act on your results
Year-round medical support, with in-chat clinician escalation
All your health records in one personal vault, with trends and biological age tracking
Early access to new diagnostics and product releases
More tests to consider
Loading essentials…
Frequently asked questions
View all FAQsHow does pricing work?
Every test shows the member price next to the standard non-member price, so you can see what membership saves you. The member price is our cost, covering the lab and what it takes to run the service. It is never a profit on the test itself. Mito makes its money on the $9 membership, not on marking up your tests. Membership is $9 per month, and any applicable lab order or draw fee is itemized before you pay.
Where do I get tested?
Choose an available partner lab at checkout. If your cart contains multiple blood tests, Mito helps consolidate the eligible tests at one lab when possible. At-home kits and scans follow the collection or appointment process shown on their product page.
Is this eligible for HSA/FSA?
Yes. Eligible tests can be paid for with an HSA or FSA card at checkout.
When will I get my results?
Your results appear in your Mito dashboard after the laboratory completes processing. A clinician then reviews them before your analysis and personalized action plan are finalized. Timing varies by test, and specialty assays and at-home kits may take longer.
Do I need a physician's order?
No. Mito provides the laboratory order when one is required, so you do not need to arrange a separate physician visit before purchasing.
Recently viewed
Loading essentials…